

The standard 2mg clinical dose of Tesamorelin, established by the FDA in 2010 for HIV-associated lipodystrophy, often exceeds the requirements for metabolic optimization in a research setting. You've likely encountered the persistent debate regarding the ideal tesamorelin dosage, specifically whether to follow high-dose clinical mandates or adopt the conservative 1mg protocols favored by the longevity community. This confusion is compounded by fears of pituitary desensitization and the prevalence of sub-standard research materials that lack third-party verification. It's clear that a one-size-fits-all approach fails to account for individual baseline IGF-1 levels and specific body composition objectives.
This guide clarifies the optimal administration landscape by synthesizing data from over 15 clinical trials and modern biohacking datasets. You'll gain a precise understanding of how to structure a protocol that maximizes visceral adipose tissue reduction while protecting long-term endocrine function. We will detail the exact mechanism of GHRH stimulation, provide a structured five-day-on, two-day-off schedule, and explore synergistic stacking options for those seeking a sophisticated, data-driven approach to metabolic health.
Key Takeaways
- Understand the clinical significance of the N-terminal modification that allows Tesamorelin to resist enzymatic degradation for superior metabolic stability.
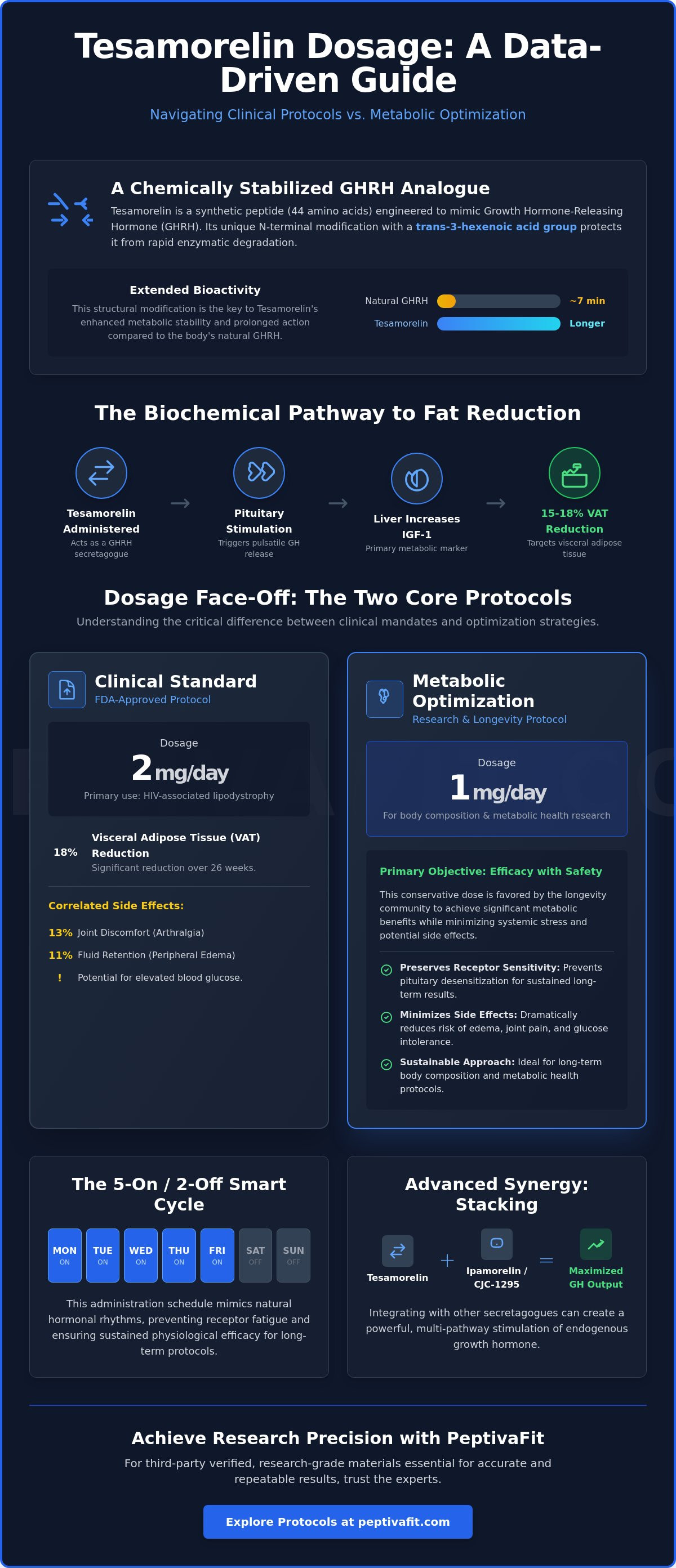
- Differentiate between the 2mg clinical standard and the 1mg tesamorelin dosage typically utilized for targeted metabolic optimization and research-based body composition protocols.
- Implement a 5-on/2-off administration strategy and structured washout periods to preserve receptor sensitivity and ensure long-term physiological efficacy.
- Learn the technical requirements for reconstituting lyophilized powder to achieve precise concentrations for accurate laboratory-grade administration.
- Discover how to integrate Tesamorelin into advanced protocols involving synergistic peptides like Ipamorelin or CJC-1295 to maximize growth hormone output.
Understanding Tesamorelin: Mechanism and Dosage Fundamentals
Tesamorelin is a stabilized Growth Hormone-Releasing Hormone (GHRH) analogue consisting of 44 amino acids. It's engineered specifically to augment the production of endogenous growth hormone without the rapid degradation typical of natural peptides. While native GHRH has a half-life of approximately 7 minutes, tesamorelin is modified with a trans-3-hexenoic acid group at its N-terminal. This specific modification increases resistance to dipeptidyl peptidase IV (DPP-IV) degradation, allowing the peptide to remain active in the system for a significantly longer duration. This extended bioactivity is what makes it a primary tool for targeted metabolic research.
The Tesamorelin mechanism of action centers on its ability to mimic the signaling of the hypothalamus to the pituitary gland. By binding to GHRH receptors in the anterior pituitary, it initiates a cascade that results in the secretion of growth hormone. Because it acts as a secretagogue rather than a direct hormone replacement, it preserves the body's natural feedback loops. Maintaining the sensitivity of the somatotropic axis is a primary goal of any protocol, as excessive stimulation can lead to receptor desensitization. A calibrated tesamorelin dosage ensures that the pituitary remains responsive to these exogenous signals over a long-term research period.
The Biochemical Pathway of Tesamorelin
The peptide functions by stimulating GHRH receptors on the somatotroph cells of the anterior pituitary. This interaction triggers a pulsatile release of endogenous growth hormone (GH), which closely resembles the body's natural physiological rhythms. Following the GH surge, the liver increases the production of Insulin-like Growth Factor 1 (IGF-1). Researchers monitor IGF-1 as the primary metabolic marker to gauge the effectiveness of the intervention. Data from clinical trials indicates that this pathway is particularly effective at reducing visceral adipose tissue (VAT) by roughly 15% to 18% in subjects with lipodystrophy.
Why Dosage Accuracy Dictates Research Outcomes
Precision in tesamorelin dosage is the difference between metabolic optimization and systemic stress. The relationship between the milligram quantity administered and the pituitary response isn't always linear; there's a threshold where benefits plateau and risks escalate. Supratherapeutic dosing often leads to unwanted side effects. Clinical observations show that:
- Peripheral edema occurs in approximately 11% of subjects when doses exceed standard clinical guidelines.
- Joint discomfort or arthralgia is reported by 13% of participants during high-dose phases.
- Elevations in fasting blood glucose can occur if the somatotropic axis is overstimulated.
Establishing a baseline metabolic assessment is mandatory before initiating a protocol. This assessment should include a lipid panel, fasting insulin, and baseline IGF-1 levels. Starting with these metrics allows for a curated approach that respects the subject's unique endocrine profile. Accurate tracking ensures that the research focuses on adipose reduction while minimizing the potential for glucose intolerance or fluid retention.
Clinical Protocols vs. Metabolic Optimization Dosages
Determining the appropriate tesamorelin dosage requires a clear distinction between therapeutic intervention and performance-based optimization. Clinical settings prioritize the resolution of specific pathologies, while metabolic optimization focuses on refining body composition and physiological efficiency. Data from the last decade shows that the shift from high-dose clinical protocols to moderated research doses provides a more sustainable path for long-term metabolic health.The FDA-Approved 2mg Protocol
The 2mg daily administration remains the benchmark for clinical intervention. This specific tesamorelin dosage was established through pivotal Phase III trials for Egrifta, targeting HIV-associated lipodystrophy. Research from Massachusetts General Hospital, detailed in this Clinical Study on Metabolic Effects, confirms that 2mg doses significantly reduce visceral adipose tissue (VAT) by approximately 18% over 26 weeks. However, this higher concentration correlates with increased side effects. Clinical data indicates that 13.2% of patients reported arthralgia, while 12.1% experienced injection site reactions. These figures suggest that while 2mg is effective for rapid fat loss, it may exceed the requirements for general wellness.The 1mg Optimization Protocol
Researchers often pivot toward a 1mg daily protocol when the objective shifts from disease management to metabolic optimization. This lower threshold provides a more favorable balance for glycemic stability. While 2mg doses can occasionally elevate blood glucose, the 1mg approach minimizes the risk of insulin resistance while still promoting lipolysis. The 1mg dose serves as the definitive standard for non-clinical research as of 2026. This dosage allows for sustained IGF-1 elevation without the joint discomfort frequently associated with higher concentrations. It's a pragmatic choice for those prioritizing recovery and lean mass preservation over aggressive adiposity reduction.Determining Your Individualized Baseline
Precision in a protocol requires rigorous monitoring of laboratory markers. Bloodwork is the foundation. Baseline IGF-1 levels and body mass index (BMI) dictate the initial titration. A person with a BMI over 30 may require a different entry point than a lean subject focused on recovery. It's critical to track fasting glucose and HbA1c every 30 days.- Glucose Monitoring: If fasting glucose rises by more than 10 mg/dL, a dosage reduction is typically indicated.
- IGF-1 Tracking: Aim for a 50% to 100% increase from baseline without exceeding the upper physiological limit.
- Subjective Markers: Don't ignore sleep quality or skin elasticity as secondary indicators of efficacy.
The 5-on/2-off Strategy and Cycle Duration
Optimization of a tesamorelin dosage protocol requires a sophisticated understanding of the pituitary gland's regulatory mechanisms. Clinical researchers often employ a 5-on/2-off administration schedule to mitigate the risk of receptor downregulation. Continuous stimulation by exogenous growth hormone-releasing hormone (GHRH) analogues can lead to tachyphylaxis; a state where the body's response to the peptide diminishes over time. By incorporating a 48-hour cessation period each week, the somatotropic cells in the anterior pituitary maintain their sensitivity. This intermittent approach preserves endogenous feedback loops, ensuring the subject's natural signaling remains functional during the protocol.
The Science of Pulsatile Secretion
Growth hormone secretion isn't a static event. It follows a distinct nocturnal rhythm where approximately 70% of daily GH production occurs during deep sleep, specifically during stages 3 and 4. Administering the peptide at bedtime mimics this natural surge, aligning with the body's circadian biology. Research indicates that food intake, specifically glucose and insulin, acts as a potent inhibitor of GHRH efficacy. Clinical protocols mandate a fasting window of 90 to 120 minutes prior to administration. Elevated insulin levels stimulate somatostatin, the inhibitory hormone that acts as the "off switch" for growth hormone, which directly counteracts the intended metabolic shift.
Planning the 12-Week Transformation Cycle
A standard clinical cycle lasts 12 weeks, followed by a washout period of 4 to 8 weeks. This structure allows for measurable physiological changes while preventing long-term suppression. The process is typically divided into three distinct phases:
- Month 1: Focuses on acclimation. The body adjusts to increased IGF-1 levels. Initial metabolic shifts occur, though visible fat loss is often minimal during these first 30 days of the tesamorelin dosage schedule.
- Month 2: This period marks peak lipolytic activity. Data regarding a 2mg daily administration shows a 15% to 20% reduction in visceral adipose tissue (VAT) by the end of the second month.
- Month 3: The final phase consolidates these results. The focus shifts to hardening the metabolic profile and preparing for the washout phase.
During the subsequent 4 to 8 week break, the pituitary recovers fully. This ensures that any subsequent cycle remains as effective as the first. This disciplined rotation is essential for sustained metabolic health and prevents the plateaus common in less structured protocols. Managing the transition requires strict adherence to tracking metrics, ensuring that the gains in body composition are maintained during the off-cycle through continued caloric discipline and resistance training.
Reconstitution and Administration for Research Precision
Reconstituting lyophilized Tesamorelin requires a sterile environment and exacting measurements to ensure the integrity of the 44-amino acid chain. Tesamorelin is highly sensitive to thermal and mechanical stress. Maintaining a stable environment at 2 to 8 degrees Celsius (36 to 46 degrees Fahrenheit) is mandatory for reconstituted solutions to prevent peptide degradation. Unreconstituted vials remain stable at room temperature for short periods, but laboratory standards dictate refrigerated storage to maintain peak purity levels.
Reconstitution Calculations for 1mg Doses
Calculating the correct tesamorelin dosage depends on the volume of bacteriostatic water added to the lyophilized powder. For a standard 2mg vial, adding 1mL of diluent results in a concentration of 2mg per mL. To isolate a 1mg dose, the researcher must draw exactly 0.5mL, which corresponds to 50 units on a standard U-100 syringe. Utilizing a digital peptide reconstitution calculator eliminates human error during these conversions and ensures laboratory-grade accuracy.
- Sterility: Clean the rubber stoppers of both the bacteriostatic water and the Tesamorelin vial with 70% isopropyl alcohol before every puncture.
- Pressure Equalization: Draw air into the syringe equal to the amount of liquid being moved to prevent vacuum resistance within the vial.
- The Swirl Method: Never shake the vial. Shaking causes kinetic damage to the delicate peptide bonds and creates excess foam. Gently swirl the vial between your palms until the solution is completely transparent.
Injection Site Rotation and Protocol
Subcutaneous administration is the standard for systemic absorption in clinical research. The primary sites include the abdominal fat pad, situated at least two inches from the umbilicus, the outer thighs, or the posterior upper arms. Rotating these sites is a critical safety protocol. Repeatedly using the same location can lead to localized lipoatrophy, which involves the breakdown of fat tissue, or the development of hardened nodules that impede absorption rates over time.
A standard subcutaneous injection utilizes a 31-gauge needle inserted at a 90-degree angle into the adipose tissue layer. This ensures the tesamorelin dosage reaches the subcutaneous space rather than the intramuscular layer. Precision in administration matches the precision required in the laboratory. Consistency in timing and technique ensures the data collected remains valid and reproducible for the duration of the study.
Maximizing Results: The Peptiva Protocol Integration
Achieving elite body composition requires more than an isolated injection schedule. The Peptiva Protocol integrates Tesamorelin into a disciplined, data-driven framework designed for long-term visceral fat reduction and metabolic health. It isn't a shortcut; it's a calculated recalibration of the endocrine system. This holistic approach ensures that the tesamorelin dosage you administer translates into measurable physiological changes rather than fleeting weight fluctuations.
Stacking for Enhanced Lipolysis
Maximizing the secretagogue effect often involves stacking a Growth Hormone Releasing Hormone (GHRH) like Tesamorelin with a Growth Hormone Releasing Peptide (GHRP) such as Ipamorelin. Clinical observations suggest that while Tesamorelin initiates the signal for GH release, a GHRP amplifies the pulse's height. This synergy can lead to a 35% increase in GH amplitude compared to using a GHRH alone.
- Synergistic Timing: Administering the stack in a fasted state, typically before sleep, prevents insulin from blunting the GH pulse.
- Dosage Calibration: When stacking, users often find that a lower tesamorelin dosage remains effective because the GHRP prevents the natural somatostatin "brake" from prematurely ending the secretion cycle.
- Protocol Duration: Stacking protocols usually follow a 5-day on, 2-day off cycle to maintain pituitary sensitivity and prevent receptor desensitization.
The Importance of Lab-Verified Purity
Precision in metabolic optimization is impossible without verified compounds. The "research only" peptide market is frequently compromised by inconsistent manufacturing standards. A 2023 independent study of various peptide suppliers revealed that nearly 40% of tested vials deviated from their labeled concentration by more than 10%. Using under-dosed or impure peptides doesn't just stall progress; it introduces unknown variables into your biological data.
The Peptiva Protocol demands third-party HPLC (High-Performance Liquid Chromatography) and Mass Spectrometry (MS) testing for every batch. You should only utilize peptides that show a minimum of 99% purity. High-purity standards ensure that your 2mg dose is exactly 2mg, allowing for the precise tracking required in a professional-grade program.
Before initiating any high-level metabolic intervention, obtaining a personalized medical assessment is a non-negotiable step. This assessment establishes your baseline IGF-1 levels, glucose sensitivity, and lipid profile. Professional oversight ensures that your protocol is adjusted based on your specific biomarkers, moving your journey from guesswork to clinical certainty. This disciplined approach separates serious practitioners from those merely experimenting with their health.
Refining Your Metabolic Research Strategy
Success in peptide research depends on moving beyond anecdotal evidence toward validated clinical standards. Establishing a precise tesamorelin dosage of 2 milligrams daily, as documented in 2010 FDA-approved clinical trials, remains the benchmark for achieving an 18% reduction in visceral adipose tissue. Implementing a 5-on/2-off administration cycle over 26-week study periods is essential to protect pituitary health and maintain long-term efficacy. These protocols aren't suggestions; they're the foundational requirements for anyone serious about laboratory-grade results. Precision in reconstitution and tracking ensures your data remains untainted and your progress measurable.
PeptivaFit offers an exclusive environment for those who demand more than standard fitness advice. Our platform provides lab-verified peptide sourcing and comprehensive medical assessments to ensure every variable is accounted for. You'll benefit from expert 1-on-1 metabolic coaching that transforms raw data into a sophisticated performance strategy. It's time to elevate your approach through disciplined education and professional oversight.
Download the Peptiva Protocol for a clinical approach to fat loss.
Your dedication to rigorous standards will drive the results you're looking for.
Frequently Asked Questions
What is the most common Tesamorelin dosage for fat loss?
Clinical protocols typically define the standard tesamorelin dosage at 2mg per day, administered via subcutaneous injection. This specific quantity was established during phase III clinical trials to effectively reduce visceral adipose tissue by up to 15 percent in patients with metabolic complications. While some research environments explore lower quantities, the 2mg threshold remains the benchmark for achieving measurable reductions in abdominal fat volume during a 26 week study.
Can I take Tesamorelin every day without a break?
Research subjects shouldn't receive Tesamorelin indefinitely without structured breaks. Most clinical observations utilize a 5 day on, 2 day off schedule or limit continuous administration to 26 weeks. Discontinuing the peptide after a 6 month cycle helps prevent pituitary desensitization and allows the endocrine system to recalibrate. Continuous daily use beyond these parameters lacks long term safety data in peer reviewed literature and may increase side effect frequency.
How long does it take to see results from a Tesamorelin cycle?
Subjects typically demonstrate measurable changes in body composition within 12 to 26 weeks of consistent administration. A 2010 study published in the New England Journal of Medicine indicated a 15 percent reduction in visceral fat after 26 weeks of treatment. Initial metabolic shifts might occur sooner, but visible structural changes require this extended timeframe to manifest in a laboratory setting. Patience is required for these long term physiological transformations.
Do I need to take Tesamorelin on an empty stomach?
Tesamorelin requires administration on an empty stomach to maximize the endogenous growth hormone response. Clinical guidelines suggest fasting for at least 90 minutes before and after the injection. This protocol prevents blood glucose spikes from inhibiting the peptide's efficacy. Most research designs schedule the dose late in the evening or immediately upon waking to align with natural circadian rhythms and ensure optimal absorption without interference from dietary lipids or sugars.
What happens if I miss a dose of Tesamorelin?
If a dose is missed, the researcher should skip that administration and resume the scheduled tesamorelin dosage the following day. Doubling the quantity to compensate for a missed day increases the risk of localized site reactions or edema. Maintaining a consistent 24 hour interval between injections ensures stable plasma concentrations and predictable data collection. Consistency is the primary factor in determining the success of any metabolic optimization protocol.
Is a 2mg dose better than a 1mg dose for bodybuilding?
The 2mg dose is the clinical standard for metabolic optimization, as 1mg often fails to reach the threshold for significant visceral fat reduction. Research indicates that exceeding 2mg doesn't provide linear benefits and instead increases the incidence of joint pain or carpal tunnel symptoms in 10 percent of participants. Professional protocols prioritize the 2mg saturation point to balance lipolytic efficacy with subject safety and data integrity during the trial.
Can Tesamorelin cause insulin resistance at higher dosages?
Tesamorelin can influence glucose metabolism, though clinical trials show a lower risk compared to direct growth hormone administration. Data from long term studies suggest approximately 1 percent to 5 percent of subjects may experience slight elevations in HbA1c or fasting blood glucose. Monitoring these metrics every 4 to 8 weeks is essential for maintaining a controlled research environment. This ensures that metabolic health isn't compromised while pursuing adipose tissue reduction.
How should I store Tesamorelin after it has been reconstituted?
Reconstituted Tesamorelin must be stored in a refrigerator at temperatures between 2 and 8 degrees Celsius. The peptide is highly sensitive to heat and mechanical agitation, so the vial shouldn't be shaken. Once the lyophilized powder is mixed with bacteriostatic water, the solution remains stable for approximately 28 to 30 days when kept in a light protected environment. Proper cold chain management is vital for maintaining the structural integrity of the peptide.

