

Most fat loss strategies fail because they ignore the precise signaling required to mobilize visceral adipose tissue without disrupting endocrine balance. You've likely reached a plateau where stubborn fat reserves remain resistant to caloric deficits, yet you remain cautious about the systemic side effects typical of non-selective secretagogues. This apprehension is scientifically justified; avoiding the hunger spikes and prolactin elevations of older GHRPs is essential for disciplined optimization. This clinical review establishes why ipamorelin for fat loss is categorized as a selective metabolic architect, leveraging endogenous growth hormone pulses to trigger targeted lipolysis.
You'll gain a structured understanding of GHRP signaling and the specific protocols required for body recomposition. We'll examine the 2026 regulatory landscape, including the WADA prohibition effective as of January 1 and the current PCAC review status. By contrasting these mechanisms with established data, such as the 15% to 18% visceral fat reduction seen in related GHRH analogues, we'll provide the criteria for identifying lab-verified research materials. This guide ensures your approach to adiposity reduction remains informed, private, and strictly data-driven.
Key Takeaways
- Understand the selective pentapeptide structure of Ipamorelin and how it functions as a ghrelin mimetic without the side effects of non-selective secretagogues.
- Discover how ipamorelin for fat loss inhibits lipoprotein lipase (LPL) to prioritize the mobilization of stubborn visceral adipose tissue.
- Evaluate the clinical rationale for stacking Ipamorelin with CJC-1295 to optimize the GHRH/GHRP axis for superior metabolic outcomes.
- Master precise protocol design, including the significance of the saturation dose and the necessity of fasted administration for molecular integrity.
- Establish rigorous criteria for identifying lab-verified research materials to ensure your protocols are free from contaminants and heavy metals.
Molecular Mechanism: Understanding Ipamorelin as a Selective GHRP
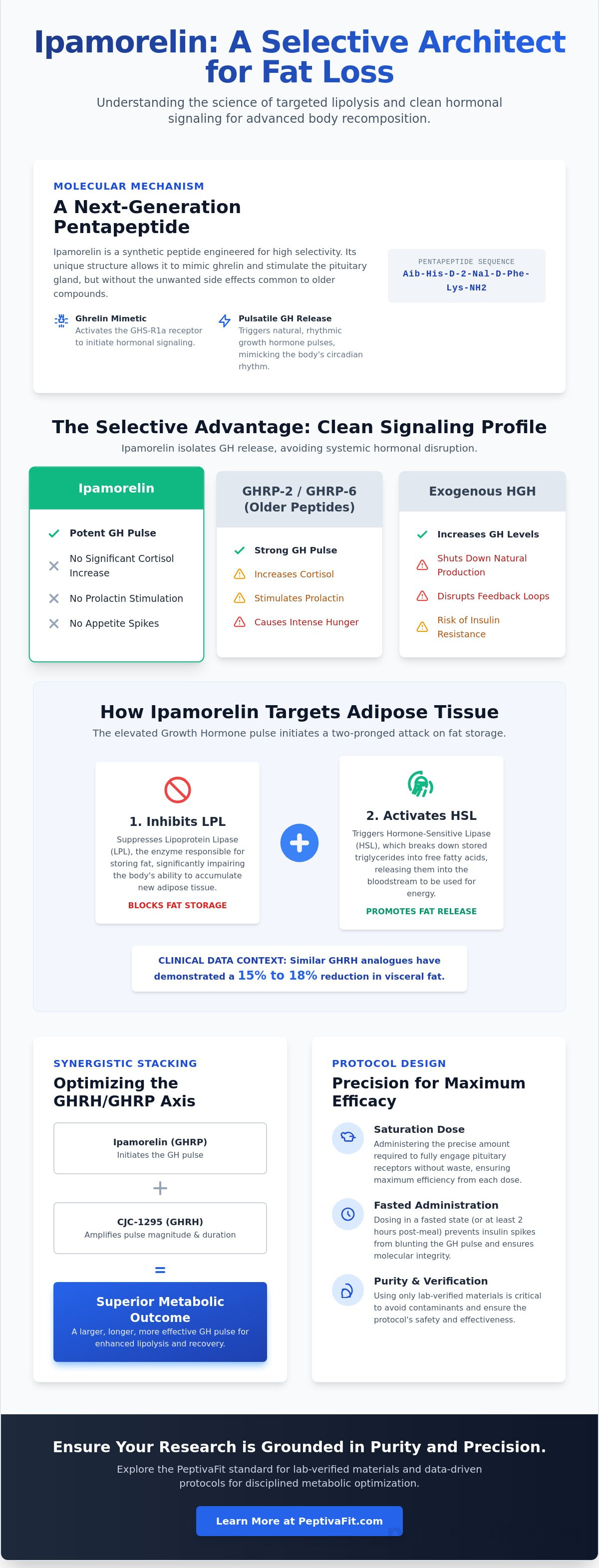
Ipamorelin represents a significant evolution in the field of growth hormone secretagogues. It is a synthetic pentapeptide with the specific sequence Aib-His-D-2-Nal-D-Phe-Lys-NH2. This precise molecular arrangement allows it to function as a highly selective ghrelin mimetic. While first-generation secretagogues often triggered unintended hormonal cascades, the strategic design of Ipamorelin ensures it binds specifically to the growth hormone secretagogue receptor (GHS-R1a) without stimulating secondary pathways. This selectivity is the primary reason researchers prioritize ipamorelin for fat loss over less refined alternatives.
The clinical advantage of this peptide lies in its clean profile. Unlike GHRP-2 or GHRP-6, which can stimulate the release of adrenocorticotropic hormone (ACTH), cortisol, and prolactin, Ipamorelin maintains a narrow focus. It triggers the somatotropes in the anterior pituitary to release growth hormone while leaving other endocrine markers virtually untouched. This makes it an ideal tool for long-term body recomposition where hormonal stability is paramount. It doesn't disrupt the delicate balance of the endocrine system.
GHS-R1a Agonism and Pituitary Signaling
By mimicking the action of ghrelin, Ipamorelin initiates a signaling cascade that results in potent growth hormone (GH) pulses. This mechanism is distinct from the aggressive appetite stimulation seen with earlier peptides. GHRP-6, for instance, frequently causes intense hunger that can compromise a fat loss protocol. Ipamorelin avoids this pitfall. It also maintains the natural pulse of GH release. Some secretagogues cause a GH bleed, where levels remain elevated in an unnatural, non-pulsatile manner. Ipamorelin works with the body’s circadian rhythm, preserving the natural ebb and flow of hormonal activity.
The Distinction from Exogenous HGH
Utilizing ipamorelin for fat loss offers a safer alternative to synthetic, exogenous Human Growth Hormone (HGH). Exogenous HGH bypasses the body's regulatory systems; it often shuts down natural GH production and desensitizes the somatostatin-GH axis. Ipamorelin encourages the body to produce its own GH instead. This preserves natural feedback loops and the inhibitory role of somatostatin. It also significantly reduces the risk of insulin resistance, which is a common side effect of high-dose exogenous HGH therapy. By maintaining insulin sensitivity, the body stays in a superior state for lipid oxidation and metabolic health.
The Science of Lipolysis: How Ipamorelin Targets Adiposity
Lipolysis is the biochemical process of breaking down triglycerides into glycerol and free fatty acids. Growth hormone (GH) acts as a primary catalyst in this metabolic sequence. When GH levels rise, the body triggers hormone-sensitive lipase (HSL) while simultaneously inhibiting lipoprotein lipase (LPL). LPL is the enzyme responsible for clearing lipids from the blood and storing them in adipose tissue. By suppressing LPL, the body's capacity to accumulate new fat is significantly impaired. This mechanism is a foundational reason why research into ipamorelin for fat loss is so prevalent in clinical settings. According to PubChem chemical data for Ipamorelin, the compound's ability to selectively stimulate GH without disrupting other metabolic markers makes it a unique candidate for long-term adiposity reduction.
Beyond direct fat breakdown, GH facilitates a process known as nutrient partitioning. This means the body becomes more efficient at directing amino acids toward protein synthesis and muscle repair rather than shunting excess calories into adipose storage. It shifts the physiological priority from metabolic storage to cellular recovery. It's this shift that allows for body recomposition, where lean mass is preserved even during a caloric deficit. For those seeking a guided approach to this metabolic transition, the Peptiva Protocol offers a structured methodology for implementing these research findings into a disciplined regimen.
Hormonal Synergy and Fat Oxidation
GH pulses specifically increase the availability of free fatty acids in the blood, which the body then utilizes for energy. This creates a sustained afterburn effect, elevating the resting metabolic rate (RMR) for hours after the initial pulse. While the GH pulse provides the immediate lipolytic signal, the subsequent rise in Insulin-like Growth Factor 1 (IGF-1) manages long-term metabolic regulation. IGF-1 supports lean tissue maintenance, ensuring that the weight lost comes predominantly from fat stores rather than functional muscle mass. This synergy prevents the metabolic slowdown often associated with standard dieting.
Visceral Fat vs. Subcutaneous Fat
Visceral fat, the deep abdominal fat surrounding internal organs, is highly metabolically active and possesses a high density of growth hormone receptors. This makes it far more responsive to GH-mediated signaling than stubborn subcutaneous fat. Reducing visceral adiposity is critical because this tissue is a primary driver of systemic inflammation and metabolic dysfunction. Many researchers find that combining ipamorelin for fat loss with AOD 9604 creates a synergistic effect. Since both peptides target fat through distinct molecular pathways without causing insulin resistance, they provide a comprehensive solution for addressing resistant abdominal deposits.
Synergistic Stacking: Optimizing the GHRH/GHRP Axis
While utilizing ipamorelin for fat loss is effective as a monotherapy, its clinical utility is maximized when paired with a Growth Hormone Releasing Hormone (GHRH). This combination addresses both sides of the hormonal equation. GHRH increases the total pool of growth hormone available in the pituitary, while the GHRP (Ipamorelin) provides the specific signal to release that pool in a concentrated pulse. This relationship creates a multiplier effect where the resulting growth hormone pulse is significantly larger than the sum of its parts. It's a strategic approach that mimics the body's endogenous signaling more accurately than single-peptide protocols.
For those prioritizing extreme abdominal fat loss, researchers often look toward Tesamorelin as the GHRH of choice. Tesamorelin has shown a unique affinity for reducing visceral adipose tissue, making it a potent substitute for CJC-1295 in specific body recomposition contexts. By optimizing the frequency and amplitude of these pulses, you can drive fat oxidation while maintaining the metabolic flexibility required for high-performance training.
The CJC-1295 + Ipamorelin Protocol
CJC-1295 without DAC (Drug Affinity Complex) is the clinical standard companion for Ipamorelin. The distinction between the "with DAC" and "without DAC" versions is critical for maintaining endocrine health. DAC creates a constant "bleed" of growth hormone that can desensitize receptors and interfere with natural circadian rhythms. The version without DAC has a shorter half-life, approximately 30 minutes, which allows for precise, pulsatile control. This timing is essential. Administering this stack before sleep or in a fasted state ensures that the exogenous signal aligns with the body's natural nocturnal GH secretion, maximizing lipolytic efficiency without causing long-term receptor downregulation.
Stacking for Recovery and Body Recomposition
Body recomposition is a multi-faceted process that extends beyond simple adiposity reduction. To support the structural demands of increased training, many protocols integrate BPC-157 for its systemic tissue repair properties. Rapid fat loss can occasionally lead to skin laxity, particularly in older demographics. In these instances, GHK-Cu is utilized to support collagen remodeling and skin elasticity. For those requiring elite-level recovery from injury or intense physical strain, the Wolverine Stack provides a comprehensive framework for simultaneous fat loss and cellular regeneration. These curated combinations ensure that as ipamorelin for fat loss works on metabolic health, the rest of the system remains structurally sound and resilient.
Protocol Design: Dosage, Timing, and Molecular Integrity
Protocol efficacy depends entirely on the metabolic environment at the time of administration. Insulin is a potent inhibitor of growth hormone release; therefore, any elevation in blood glucose will neutralize the secretagogue's effect. A strict fasting window of 2 to 3 hours before and after administration is required to ensure the pituitary response isn't blunted by caloric intake. This discipline is the cornerstone of utilizing ipamorelin for fat loss successfully. Research-only protocols often emphasize a nocturnal administration to align with the body's natural circadian GH release, though a secondary morning dose is frequently utilized in advanced body recomposition settings.
The concept of a 'saturation dose' is central to clinical research. Evidence suggests that the GHS-R1a receptors reach a point of maximal stimulation at approximately 1mcg per kg of body weight. Exceeding this threshold rarely results in additional growth hormone secretion and may instead increase the risk of receptor desensitization. A disciplined approach prioritizes precision over quantity. Clinical result timelines typically begin with improved sleep quality and recovery within the first 14 days, followed by measurable shifts in resting metabolic rate by week 6. Visible changes in targeted adiposity generally require 12 to 16 weeks of consistent adherence to the protocol. For those requiring professional guidance to navigate these variables, a personalized medical assessment ensures your strategy is built on data rather than speculation.
Administration and Reconstitution Standards
Maintaining the structural stability of the peptide is paramount. Researchers must understand how to reconstitute peptides using bacteriostatic water to prevent bacterial growth and molecular degradation. Once reconstituted, Ipamorelin is highly sensitive to temperature and agitation. It must be stored in refrigerated conditions between 2°C and 8°C (36°F to 46°F) and typically retains its molecular integrity for 21 to 28 days. Administration is performed via subcutaneous injection into the adipose tissue, usually in the abdominal region, where it is slowly absorbed into systemic circulation.
Managing Potential Side Effects
While Ipamorelin is celebrated for its selectivity, some researchers report transient water retention during the initial phase of a protocol. This is often mitigated by managing the sodium-to-potassium ratio and ensuring adequate hydration. In rare instances, a slight tingling sensation in the extremities, similar to mild carpal tunnel symptoms, may occur if GH levels rise too rapidly. To prevent receptor downregulation and maintain the sensitivity of the GHS-R1a pathway, a cycling protocol is highly recommended. A common standard is the 5 days on, 2 days off approach, which allows the pituitary gland to maintain its endogenous rhythm while preventing the diminishing returns associated with chronic, uninterrupted stimulation.
The Peptiva Standard: Lab-Verified Purity and Professional Oversight
The efficacy of ipamorelin for fat loss is contingent upon the biochemical integrity of the compound utilized. Within the unregulated digital marketplace, the term 'research grade' is often used as a legal shield rather than a mark of quality. There is a significant distinction between a peptide that is merely available and one that is lab-verified for human-grade research. Substandard materials frequently contain residual solvents, acetates, or heavy metals such as lead and arsenic. These contaminants don't just hinder fat loss; they can trigger systemic inflammatory responses that compromise your entire metabolic profile.
PeptivaFit operates as a curated gatekeeper in this space. We recognize that sophisticated performance optimization requires more than just access to molecules; it demands laboratory-grade standards. Every protocol we provide is built on the foundation of lab-tested peptides, ensuring that the molecular sequence is exactly what is stated on the vial. Beyond the substance itself, a personalized medical assessment is required to establish your baseline endocrine health. This ensures that your approach to ipamorelin for fat loss is grounded in your specific physiological data, rather than generic internet hearsay.
How to Read a Certificate of Analysis (COA)
A legitimate Certificate of Analysis (COA) is the only way to verify molecular stability. You must look for High-Performance Liquid Chromatography (HPLC) data, which is the gold standard for determining purity levels. A purity percentage below 99% is unacceptable for clinical-grade research, as the remaining 1% often consists of unknown peptide fragments or synthesis byproducts. Mass spectrometry should also be present to confirm the exact molecular weight of the pentapeptide. Be wary of static PDF documents that lack a verifiable batch number or a digital signature from an independent third-party laboratory.
The Role of Professional Coaching
Scientific optimization isn't a static event; it's a dynamic process that requires constant tracking. Relying on subjective "feeling" is insufficient when managing growth hormone secretagogues. Professional 1-on-1 coaching provides the external oversight needed to interpret bio-feedback, such as shifts in resting heart rate, sleep architecture, and glucose sensitivity. This data-driven approach allows for the precise adjustment of dosages and timing, ensuring the GHS-R1a receptors remain responsive. You can achieve your body composition goals with the Peptiva Protocol by integrating these high-level standards into a disciplined, professionally managed regimen.
Implementing Data-Driven Adiposity Reduction
Successful body recomposition requires a transition from generic dieting to precise hormonal management. This review has established that ipamorelin for fat loss operates through highly selective GHS-R1a agonism, avoiding the systemic disruptions common in earlier peptide generations. By leveraging the synergistic relationship between GHRH and GHRP signaling, you can mobilize stubborn visceral fat while preserving functional lean mass. These mechanisms ensure that your metabolic environment remains optimized for long-term health rather than temporary weight loss.
Achieving these clinical result timelines depends on the integrity of your materials and the discipline of your protocol. PeptivaFit provides the necessary framework for this evolution through lab-verified peptide supplies and personalized medical assessments. Our approach replaces speculation with data, ensuring your metabolic optimization is both safe and efficient. You'll benefit from a curated environment where privacy and expertise are the standard.
Optimize your metabolism with the Peptiva Protocol and lab-tested peptides to begin your structured transformation. With expert 1-on-1 coaching, you'll have the oversight required to navigate the complexities of peptide research with absolute confidence. It's time to take sophisticated control of your performance and wellness.
Frequently Asked Questions
How long does it take to see fat loss results with Ipamorelin?
Visible changes in adiposity typically require 12 to 16 weeks of consistent adherence to a protocol. While initial improvements in sleep and recovery quality often occur within the first 14 days, the metabolic shifts necessary for targeted lipolysis take longer to manifest. Measurable changes in resting metabolic rate generally become evident by week 6 of a disciplined regimen.
Do I need to follow a specific diet while using Ipamorelin for fat loss?
A high-protein, calorie-controlled diet is essential to maximize the effects of ipamorelin for fat loss. While the peptide facilitates the mobilization of free fatty acids, it can't overcome a significant caloric surplus. The most critical dietary factor is the timing of your meals; you must avoid carbohydrates and fats during the administration window to prevent insulin from blunting the growth hormone pulse.
Can Ipamorelin cause a failed drug test for athletes?
Ipamorelin will cause a failed drug test for any athlete subject to World Anti-Doping Agency (WADA) regulations. As of January 1, 2026, it's explicitly named on the Prohibited List under section S2 as a peptide hormone mimetic. This prohibition is effective for both in-competition and out-of-competition testing across all sanctioned athletic organizations.
What is the difference between Ipamorelin and CJC-1295?
Ipamorelin is a Growth Hormone Releasing Peptide (GHRP) that triggers the immediate release of growth hormone, while CJC-1295 is a Growth Hormone Releasing Hormone (GHRH) that increases the production and total pool of GH. They operate on distinct receptors within the pituitary gland. Stacking them creates a synergistic effect that results in a significantly larger GH pulse than using either peptide as a monotherapy.
Is Ipamorelin safe for long-term use in metabolic optimization?
Long-term clinical use requires a disciplined cycling strategy to maintain receptor sensitivity and endocrine balance. Most research protocols suggest a "5 days on, 2 days off" schedule to prevent the pituitary gland from becoming desensitized to the signal. It's also vital to monitor the ongoing PCAC review regarding its status in compounding pharmacies to ensure your research remains compliant with 2026 regulations.
Will Ipamorelin make me feel hungry like GHRP-6?
Ipamorelin doesn't cause the intense hunger spikes associated with GHRP-6 because of its selective molecular structure. It's a refined secretagogue that targets the GHS-R1a receptor without stimulating the gastric pathways that trigger appetite. This selectivity makes ipamorelin for fat loss a superior choice for individuals who need to maintain a strict caloric deficit without the distraction of increased ghrelin signaling.
What happens if I eat immediately after an Ipamorelin administration?
Consuming food immediately after administration will effectively neutralize the growth hormone pulse. Insulin is the primary physiological inhibitor of GH secretion; any rise in blood glucose will blunt the pituitary gland's response. You must adhere to a strict 2 to 3 hour fasting window before and after each administration to ensure the molecular signaling remains effective.
How should I store Ipamorelin to maintain its molecular integrity?
You must store reconstituted Ipamorelin in a refrigerated environment between 2°C and 8°C (36°F to 46°F). Exposure to room temperature for extended periods or direct sunlight will cause rapid molecular degradation. Once the lyophilized powder is reconstituted with bacteriostatic water, it generally maintains its structural integrity for 21 to 28 days if kept cold and handled without aggressive agitation.

